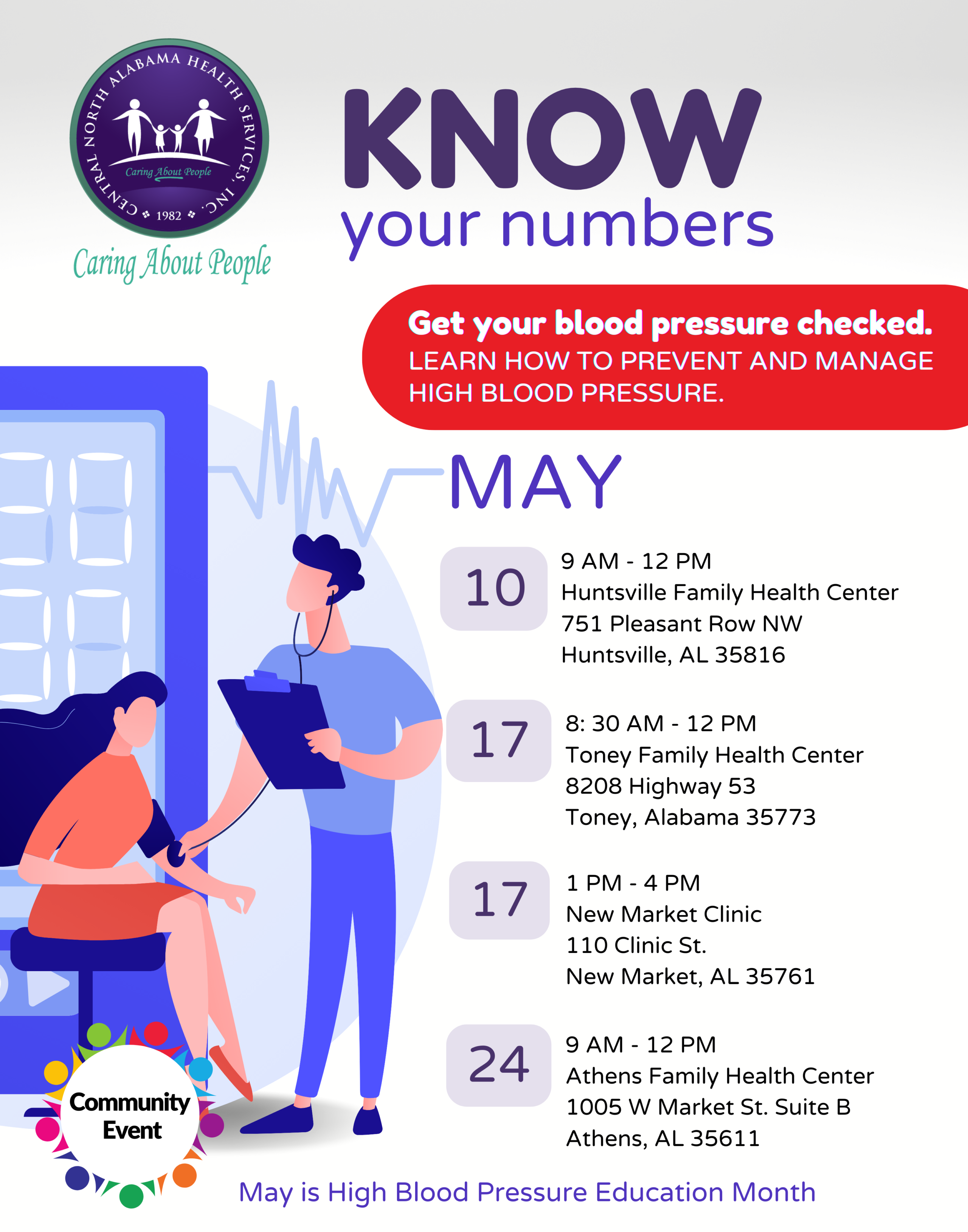
May is National High Blood Pressure Education Month
Only about 1 in 4 people withHigh Blood Pressurehave their condition under control.
As people in the United States come to terms with their second year of COVID-19, a new campaign is reminding them to make cardiovascular health a priority, especially during the pandemic. The “Start Small. Live Big.” campaign will encourage adults, particularly those 55 and older, to get back on track with the small steps—like scheduling their medical appointments, getting active, and eating healthy—so that they can get back to living big. We are happy to join with the CDC Foundation, the Million Hearts® initiative, and organizations across the nation in sharing these important messages.
"High blood pressure puts you at an increased risk for heart disease, heart failure, and stroke, among other things."
Annemarie Witmer, CRNP
Start Small. Live Big!
Join us this month for heart healthy events!
These free events are open to our patients and the public.
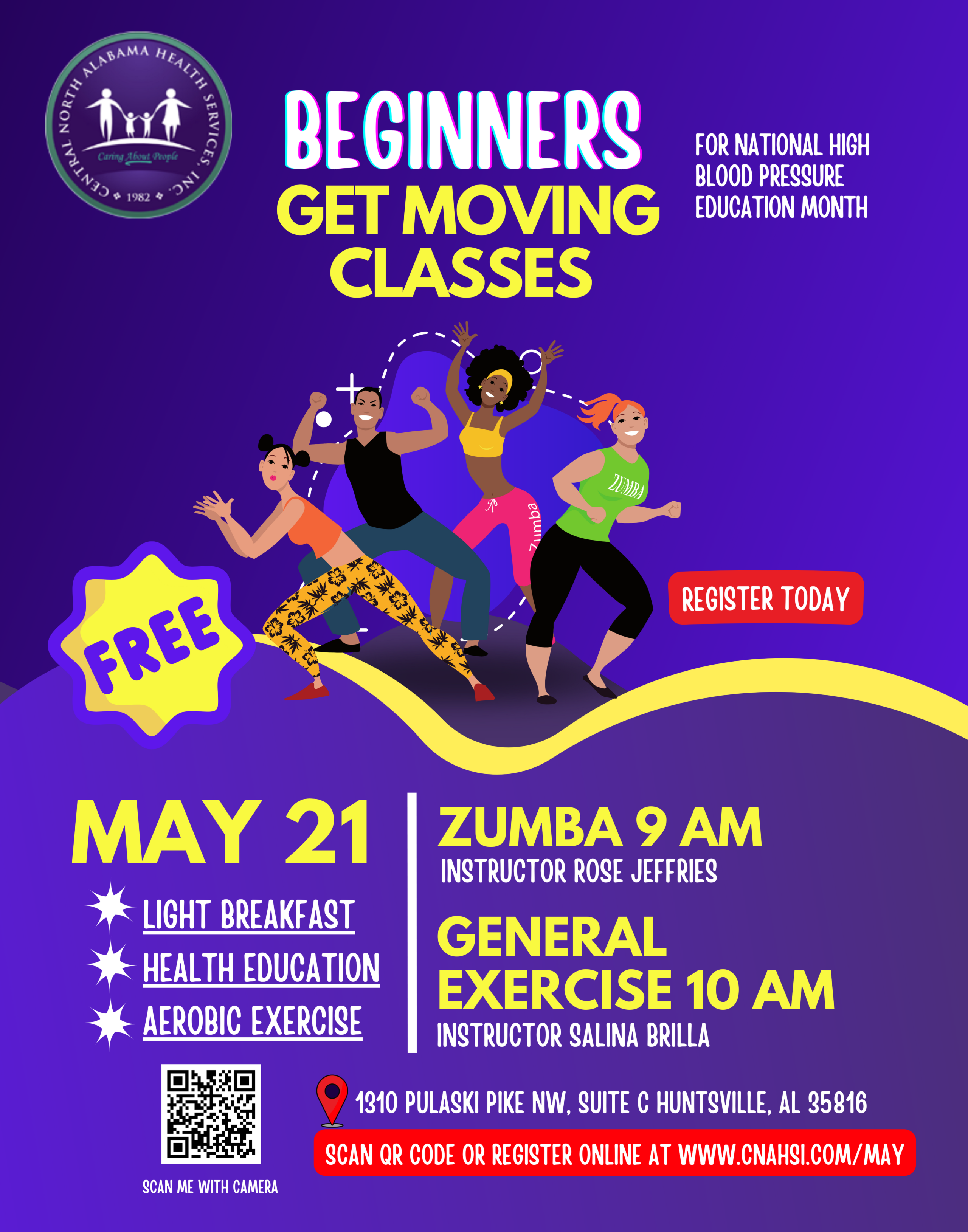
Getting active doesn’t have to be overwhelming. Join us May 21, 2022 for a beginner’s “Get Moving” class. These classes are beginner level sessions intended for ages 13 and up and for those who do little to no exercise. Space is limited, register today!
Register – Get Moving Class
Small Steps for a Healthy Heart!
You can make small steps today!
A big life is made up of the small things you do – like visiting your health care professional to take back control of your heart health. Learn more about taking small steps today!
May is National High Blood Pressure Education Month
Only about 1 in 4 people withHigh Blood Pressurehave their condition under control.
As people in the United States come to terms with their second year of COVID-19, a new campaign is reminding them to make cardiovascular health a priority, especially during the pandemic. The “Start Small. Live Big.” campaign will encourage adults, particularly those 55 and older, to get back on track with the small steps—like scheduling their medical appointments, getting active, and eating healthy—so that they can get back to living big. We are happy to join with the CDC Foundation, the Million Hearts® initiative, and organizations across the nation in sharing these important messages.
"High blood pressure puts you at an increased risk for heart disease, heart failure, and stroke, among other things."
Annemarie Witmer, CRNP
Start Small. Live Big!
Join us this month for heart healthy events!
These free events are open to our patients and the public.
Getting active doesn’t have to be overwhelming. Join us May 21, 2022 for a beginner’s “Get Moving” class. These classes are beginner level sessions intended for ages 13 and up and for those who do little to no exercise. Space is limited, register today!
Register – Get Moving Class
Small Steps for a Healthy Heart!
You can make small steps today!
A big life is made up of the small things you do – like visiting your health care professional to take back control of your heart health. Learn more about taking small steps today!